Do I need knee surgery?
The knee is a complex hinge joint. Here is a diagram to help name the parts:
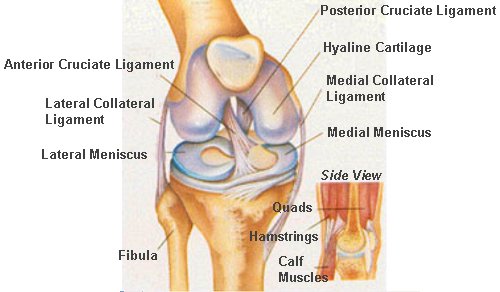
Knee surgery is broadly divided into arthroscopic (keyhole) surgery and joint replacement surgery. Joint replacement is usually considered in older patients when the joint (hyaline) cartilage is worn down to the underlying bone. Arthroscopic surgery is used more commonly in younger patients to address problems with the soft tissues within and around the knee, such as a torn cartilage (meniscus) or ligament. There is a middle ground where arthroscopic microfracture, osteotomy (leg re-alignment) or limited joint replacement (through minimally invasive surgery MIS) may be considered.
Alternative therapies may be employed first and include;
Physiotherapy: - to regain muscular control and aid relief through manipulation, taping, ultrasound and other techniques.
Medication: - painkillers, NSAIDs, cortisone or viscosupplementation (hyaluronic acid) injection
Bracing: - functional, such as the ACL brace or 'offloader' brace.
Other therapies have a role and include: dietary (glucosamine/chondroitin sulphate), acupuncture, osteopathy, reflexology, homeopathy, magnetotherapy and aromatherapy.
KNEE ARTHROSCOPY
Keyhole surgery is not new - the first keyhole operation on the knee was performed in 1918, peering down a hollow tube with the naked eye. It was difficult to see properly and nearly impossible to operate down the tube. Thankfully, the development of video, fibre optics and micro-instruments in the last 20 years has allowed the technique to become widely adopted. Its use for 'day-case' surgery and its low complication rate have revolutionised orthopaedic practice.
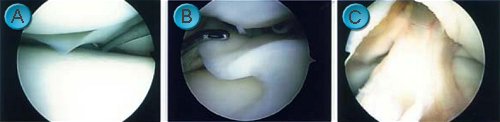
An excellent view of the inner workings of the knee can be obtained (
A: normal meniscus (cartilage),
B: torn meniscus,
C: normal anterior cruciate ligament (ACL)).
Complex surgery can also be undertaken (
D: meniscal repair,
E: ACL reconstruction,
F: microfracture).

The technique is however technically demanding, requiring expensive equipment and in certain situations access can limit its usefulness.
What will happen to me?
Usually you will be asked to come to hospital on the day of surgery, having had nothing to eat or drink since midnight. The operation can be performed under local or general anaesthetic. Some patients opt to watch the operation 'live' on the theatre television. Often photographs and a video can be taken if you decide to be asleep. After surgery you will have a firm bandage around your knee and after a few hours, be encouraged to walk and bend the leg. At this point you will be allowed home. The bandage can be removed at 48hours and you will be given an elasticated stocking to wear. Driving may be allowed at this time. The two small sticking plasters over the keyhole wounds are removed on the fifth day. Stitches are not normally required. By two weeks the discomfort should be much improved as you return to normal activities, though some symptoms (such as swelling) persist for a month or so. Physiotherapy is provided during this time, with return to sport at around a month. Any symptoms you have at three months are likely to remain.
The above relates to routine minor arthroscopic surgery and will be different in more complex cases (e.g. meniscal repair, microfracture, ACL reconstruction).
Complications
These are uncommon and are divided into those at the time of surgery and post-operative. Injury to small nerves and blood vessels at the keyholes can lead to local skin numbness or bleeding. Injury to the major nerves or blood vessels (usually by the tourniquet) is rare (<0.5% cases) and normally resolves within a few hours. Instrument failure or an incomplete procedure (e.g. if the space is tight) occurs occasionally and is procedure specific. In the post operative period there is a chance of a blood clot (DVT / PE) ~5%, bleeding (haemarthrosis) ~1%, infection ~0.2%.
Further surgery may be required in certain conditions
Here are a few examples: 23% of patients who undergo meniscal surgery require further resection; in combined ACL and meniscal injuries, dealing with the meniscus alone will improve symtoms in 84%, but 10% will be worse 4 � years later; 10% of ACL reconstructions stretch out or fail over time; arthroscopic washout provides worthwhile relief for early arthritis at 5 years in ~75%, though this is reduced if the knee is deformed.
What to do next?
Please see the end of Hip Guides
KNEE REPLACEMENT
Originally far fewer knee replacements compared to total hip replacements were performed. This trend is now reversing due to design improvements - around 12,000 / year are performed in the UK alone - now with good long term results similar to total hip replacements, around 90% still functioning at 10 years.
Knee replacements come in all sorts of shapes and sizes, but are broadly separated into total (TKR) or half (uni-compartmental - UKR) knee replacements. TKR's resurface the whole femur (thigh bone) and tibia (shin bone) with metal and have a plastic bearing between the two (
A: arthritic knee,
B: total knee replacement).

UKR's typically resurface the medial (inner) half of the knee (C: front view, D: side view), though there are implants available for the lateral (outer) half and the patello-femoral (kneecap) joint.
 What will happen to me?
What will happen to me?
You will usually be seen a week or two prior to surgery in a pre-assessment clinic for blood tests, heart / lung and general fitness testing. You may be admitted the afternoon before surgery or in the morning if your operation is not until later in the day, to allow blood pressure monitoring etc. Most patients have local anaesthetic injected into the lower back (Spinal or epidural anaesthetic) in combination with sedation. Your surgery will be performed in a sterile environment in theatre with ultra clean laminar airflow, to reduce the risk of infection. After surgery you will have numb legs for several hours, which helps with pain relief. You will have a large bandage around the knee and lower leg. The following day feeling and movement (and pain) gradually returns and you will be given painkillers to allow you to begin exercising. An X-ray will be taken. On the second day you will begin exercising in earnest, bending the knee and walking. Usually by day 6 you will be able to manage stairs and ready for discharge home. The knee will bend around 70-90 degrees, with further improvement over the subsequent days and weeks, ultimately bending around 110 degrees. The final bend depends more on how much it bent before surgery, than on the surgery itself. Outpatient physiotherapy will be arranged. By six weeks you will be off walking supports and able to drive. Full recovery usually takes about 3 months. Contact sports are discouraged, such as running or jumping.
Complications
Overall these are uncommon, typically occurring in ~5% of procedures. They are more common with advancing age and in patients with other ailments, such as diabetes or heart disease. Urinary retention requiring catheterisation, stiffness, wound healing problems, haematoma and blood clots account for most of these. Infection, though rare (~1%) can be a disaster as the knee replacement may need to be removed. It is common to experience a numb patch of skin to the side of the knee. Thankfully more serious nerve or blood vessel damage is rare (<1%).
Results
Good long term results for total knee replacements can now be expected, with around 90% still functioning at 10 years. Unicompartmental success is lower, around 80% at 10 years, although revision may be easier. Revision knee surgery is more complex, with greater risk and poorer long term outcome, compared to primary surgery.
There is a lot of debate as to whether the patella (kneecap) should be resurfaced during total knee replacement surgery. In large randomised studies looking at this issue, there is little difference, both groups having symptoms related to the patella in ~5% of cases at 10 years. Our practice is to resurface in selected cases.
What to do next?
Please see the end of Hip Guides